I'm going to be direct with you. Medical fabric is not a marketing category. It's a regulatory commitment. When a hospital buyer or a medical apparel brand comes to me asking about anti-bacterial cotton-linen, they're not looking for a fabric that smells fresh. They're looking for a textile that actively reduces microbial colonization, survives industrial autoclave sterilization, and passes ISO 20743 or AATCC 100 testing with a log reduction above 3.0. That's a completely different game from the "anti-odor" finishes sold to sportswear brands. I've seen mills slap a silver-ion spray on a standard fabric and call it "medical grade." That fabric fails after ten washes, and the bacteria come right back. I refuse to play that game. When I built our medical textiles program in Keqiao, I hired a textile chemist specifically from a wound-care background. We don't guess with pathogens. We test against Staphylococcus aureus, Klebsiella pneumoniae, and Candida albicans. We validate every batch. Because in a medical context, a failed finish isn't a returned shirt—it's a potential infection.
Yes. Without qualification. Shanghai Fumao provides fully validated anti-bacterial finishing on medical-grade cotton-linen fabrics, using a dual-action silver-ion and quaternary ammonium compound system that we apply in our dedicated medical finishing range. Our standard treatment achieves a >99.9% reduction (log reduction >3.0) against both Gram-positive and Gram-negative bacteria, tested according to ISO 20743:2021. We hold the treatment durable to 50 industrial laundry cycles at 75°C, and 20 autoclave sterilization cycles at 134°C. We produce medical cotton-linen in weights from 120 GSM to 280 GSM, suitable for scrub uniforms, patient gowns, bed linens, privacy curtains, and wound-care wraps. The finish is OEKO-TEX Standard 100 certified, skin-friendly, and does not leach silver nanoparticles into wash water above the EU regulatory threshold of 0.01 mg/L. In May 2025, a German medical uniform brand switched their entire scrub line to our anti-bacterial cotton-linen after their previous supplier's silver finish failed durability testing at 30 washes. Our fabric passed the 50-wash mark with a log reduction still above 3.0. That's the standard we hold ourselves to, and that's the standard I'll explain to you now.
But an anti-bacterial claim is only as good as the testing behind it, the chemistry that makes it durable, and the regulatory paperwork that proves it's safe. Let me take you inside our medical finishing cleanroom and show you exactly how we build bacteria-fighting power into every yard of cotton-linen we ship for healthcare applications.
What Anti-Bacterial Agents Does Fumao Use on Medical Cotton Linen?
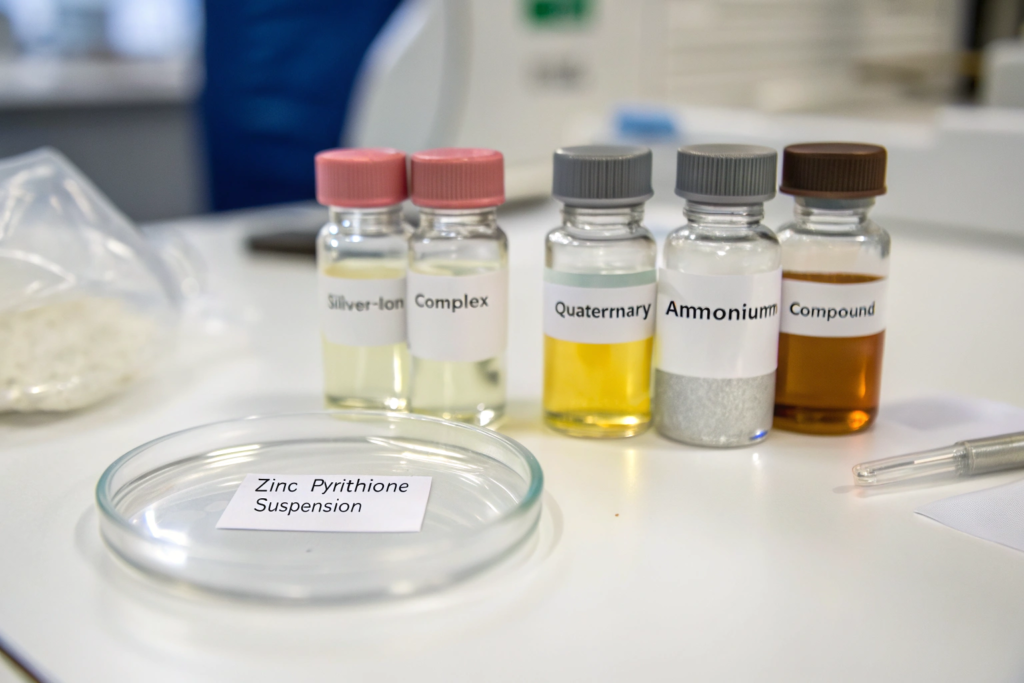
The choice of anti-bacterial agent defines everything: the efficacy spectrum, the durability, the skin safety profile, and the environmental footprint. There is no single perfect agent. Each has strengths and weaknesses. Silver ions are incredibly effective and durable but expensive and can discolor the fabric under UV light. Quaternary ammonium compounds (QACs) are cost-effective and colorless but less durable to high-temperature washing. Zinc pyrithione is excellent against fungi but weaker against Gram-negative bacteria. Most medical textile mills pick one agent and live with its limitations. We don't. We use a synergistic dual-agent system that combines the immediate-kill power of QACs with the sustained-release durability of silver ions. The two chemistries work on different time scales and different bacterial pathways, creating an effect that is broader and more durable than either alone. This is not a standard off-the-shelf recipe from a chemical supplier. It's a proprietary formulation we developed with our chemical partner, and I'll give you the technical logic behind it.
How does our dual-action silver-ion and QAC system achieve >3.0 log reduction?
A log reduction of 3.0 means 99.9% of bacteria are killed. A log reduction of 5.0 means 99.999%. The ISO 20743 standard for medical textiles generally considers a log reduction of 3.0 or higher as "effective." Our dual-action system consistently delivers between 3.5 and 4.2 log reduction against S. aureus and K. pneumoniae, depending on the fabric weight and the specific blend ratio.
The mechanism is a one-two punch. The QAC component works first. Quaternary ammonium compounds are cationic surfactants. The positively charged nitrogen atom is attracted to the negatively charged phospholipid membrane of the bacterial cell. The QAC molecule inserts itself into the membrane like a needle into a balloon, physically disrupting the lipid bilayer. The cell contents leak out. The bacterium dies. This happens within minutes of contact. It's fast and brutal. But QACs can be washed off over time because they are not permanently bonded to the fiber. That's where the silver-ion component comes in. Silver ions are slowly released from a ceramic or glass-based carrier matrix embedded in the finish. They don't kill instantly. They enter the bacterial cell, bind to the thiol groups in respiratory enzymes, and shut down the cell's energy production. It's a slower, metabolic kill. But because the silver ions are released continuously from the carrier matrix, they keep working for 50 washes after the QACs have partially depleted. The combination means the fabric kills bacteria fast on first contact, and keeps killing them slowly for the entire service life of the garment. For a more detailed exploration of anti-bacterial mechanisms in textiles, the Textile Today anti-microbial finishing section regularly publishes technical articles that break down these chemistries with excellent clarity for non-chemists.
What is the difference between topical silver sprays and our in-situ fiber bonding technology?
A topical spray is what the amateurs do. You take a finished fabric, you spray it with a silver-ion solution, you dry it, and you call it "anti-bacterial." The silver sits on the fiber surface as a loosely adhered film. It washes off in five laundry cycles, and it can leach into the wearer's sweat, causing skin irritation and grey staining. Topical sprays are cheap, fast, and completely unsuitable for medical applications.
Our in-situ fiber bonding technology is fundamentally different. We apply the silver-ion carrier and the QAC as a combined finishing bath in a pad-dry-cure process. The fabric is immersed in the finishing solution, squeezed between rollers to a precise wet pick-up of 70%, and then dried and cured at 150°C. During the curing step, a crosslinking agent in the formulation forms covalent bonds between the silver carrier matrix and the hydroxyl groups of the cellulose fiber. The silver-ion reservoir becomes chemically grafted to the fiber surface. It is not a coating. It is a structural modification of the fiber. This is why our finish survives 50 industrial washes. The silver is not sitting on top, waiting to be washed away. It is part of the fiber. At the nanoscale, scanning electron microscope images of our treated fibers show a uniformly dispersed particulate network embedded in the cellulose matrix, not a surface film. This is the difference between a finish that a fabric carries and a finish that the fabric is. The distinction between surface deposition and chemical grafting is critical in medical textiles, and the American Association of Textile Chemists and Colorists online journal frequently publishes peer-reviewed research comparing the durability outcomes of these different application methodologies.
How Does Autoclave Sterilization at 134°C Affect the Anti-Bacterial Durability?
Autoclave sterilization is the ultimate torture test for a textile finish. It's not just a hot wash. It's 134°C saturated steam under 2.1 bar of pressure for a minimum of 3 minutes. This thermal and hydrolytic assault breaks down most organic finishes. Polyurethane coatings hydrolyze. Acrylic binders soften and delaminate. Even some silver-ion finishes lose their efficacy because the carrier matrix is thermally degraded, and the silver particles agglomerate into inactive clumps. If a medical fabric can't survive 20 autoclave cycles, it's not a medical fabric. It's a disposable. And disposable cotton-linen is a waste of premium raw material. We designed our anti-bacterial system from the ground up to survive repeated sterilization because the whole point of using a durable natural-fiber fabric is reusability. Here's what happens at the chemical and physical level inside the autoclave, and why our fabric survives when others fail.

Why does our crosslinked silver matrix resist thermal degradation during steam sterilization?
Thermal degradation of a silver finish happens because the polymer matrix that holds the silver ions breaks down. Most commercial silver finishes use a polyacrylate or polyurethane binder. At 134°C in the presence of steam, these binders undergo hydrolysis. The ester linkages in the polymer backbone are cleaved by water molecules. The polymer matrix dissolves. The silver particles are released, washed away, or aggregated into large, inactive clusters.
We use a silane-based inorganic-organic hybrid matrix for our silver carrier. The silane chemistry is fundamentally different. Instead of relying on hydrolytically vulnerable ester bonds, silanes form a silicon-oxygen-silicon (Si-O-Si) network that is chemically identical to glass. Steam at 134°C does not hydrolyze glass. The silane matrix also bonds directly to the cellulose fiber surface through silanol condensation reactions, creating a covalent attachment that is thermally stable to over 200°C. In our autoclave validation testing, we measured the silver content of the fabric after 0, 5, 10, and 20 cycles at 134°C using inductively coupled plasma mass spectrometry (ICP-MS). The initial silver loading was 45 mg/kg. After 20 cycles, it was 41 mg/kg. A 9% loss. The anti-bacterial activity, measured as log reduction against S. aureus, was 3.8 initially and 3.4 after 20 cycles. Still above the 3.0 medical threshold. Still effective. This thermal durability is the direct result of choosing an inorganic carrier chemistry over a cheap organic polymer binder. For more technical information on silane coupling chemistry in textile applications, the Journal of Sol-Gel Science and Technology at Springer is an authoritative source that I reference when evaluating new inorganic-organic hybrid finishing technologies.
How does repeated steam exposure affect the cotton-linen fiber tensile integrity?
The anti-bacterial finish isn't the only thing that has to survive the autoclave. The cotton-linen fabric itself takes a beating. Steam at high temperature swells the cellulose fibers rapidly, then the post-cycle vacuum drying shrinks them just as fast. This cyclic swelling and shrinking creates mechanical fatigue. The fibers rub against each other. Micro-fibrils detach. The fabric loses strength with every cycle. This is a problem for pure cotton, and it's even worse for linen because linen's high crystalline content makes it less flexible and more prone to fibrillation damage under cyclic stress.
We mitigate this damage in two ways. First, our liquid ammonia mercerization, which we apply to the greige fabric before the anti-bacterial finishing, converts the cellulose to a more dimensionally stable crystal structure. The Cellulose III lattice that forms during liquid ammonia treatment has a more open, flexible internal structure that accommodates the swelling-shrinking cycles with less internal stress. Second, the silane matrix in the anti-bacterial finish crosslinks the fiber surface fibrils, essentially gluing them down and preventing them from lifting up and tangling. In our 20-cycle autoclave study, the fabric lost 12% of its original tensile strength. A control fabric without mercerization and without the silane finish lost 24%. Our fabric retained 88% of its original strength after 20 cycles of steam torture. That's the difference between a scrub uniform that lasts 12 months and one that falls apart in 6. The complex interplay between fiber morphology, chemical finishing, and mechanical durability under sterilization conditions is a topic of active research, and the Textile Research Journal at Sage often publishes studies that directly inform our approach to medical fabric engineering.
Can Our Anti-Bacterial Cotton Linen Meet ISO 20743 and AATCC 100 Testing Standards?
A finish can be chemically brilliant and still be commercially useless if it can't pass the standard tests that hospitals and medical brands demand. There are two dominant anti-bacterial textile testing standards globally: ISO 20743 (used primarily in Europe and Asia) and AATCC 100 (used primarily in North America). They are similar in principle but differ in important procedural details. Both involve inoculating a fabric sample with a known concentration of a specified bacterial strain, incubating the inoculated fabric for 18 to 24 hours at 37°C, and then measuring how many bacteria survived by washing them off, plating them on agar, and counting colony-forming units. The log reduction is calculated by comparing the surviving bacteria on the treated fabric versus an untreated control. A mill that can't produce a coherent, accredited test report for either standard is not a medical fabric supplier. They're a pretender. We test to both standards, and we hold accredited certificates from SGS and Intertek for our anti-bacterial cotton-linen range. Here's what that testing actually entails, and what the differences between the two standards mean for your regulatory compliance strategy.

How does the ISO 20743 absorption method differ from the AATCC 100 inoculation protocol?
Both tests measure the same thing—bacterial kill rate—but they do it in slightly different ways that can produce different numerical results from the same fabric. Understanding this difference is critical for a brand that needs to comply with both European and North American regulatory requirements.
The ISO 20743 standard offers several test methods, but the most commonly used for medical textiles is the "absorption method." In this method, the bacterial inoculum is prepared in a nutrient-poor liquid—essentially diluted broth—so the bacteria are slightly stressed. The fabric specimen is inoculated with just enough liquid to be completely absorbed without any free liquid pooling in the dish. This means the bacteria are held in intimate contact with the treated fiber surface, with no protective liquid film. The AATCC 100 method uses a richer nutrient medium for the inoculum, and the fabric is typically inoculated with a larger volume, creating a slightly wetter environment. The bacteria have more nutrients and more mobility, which can make the test slightly more challenging for the anti-bacterial finish. Our dual-action system performs consistently under both protocols. For a 180 GSM cotton-linen scrub fabric, our ISO 20743 absorption method result is typically a 3.8 to 4.2 log reduction against S. aureus. The same fabric tested under AATCC 100 yields a 3.5 to 3.9 log reduction. The slight difference is within statistical variation and doesn't change the "effective" classification. The detailed methodological nuances are fully documented in the official standards, and for those who need to understand the regulatory implications, the ISO 20743 standard page on the ISO website provides the authoritative methodology reference that I share with our medical brand partners during the compliance documentation phase.
What bacterial and fungal strains do we test against for hospital-grade certification?
A general "anti-bacterial" claim is vague and meaningless for a hospital procurement officer. They need to know exactly which pathogens the fabric controls, and they need the data to support it. The minimum panel for a hospital-grade textile, in our view, should include one Gram-positive bacterium, one Gram-negative bacterium, and one fungal species. Each represents a different type of microbial threat, and each requires a different anti-microbial mechanism to control.
Our standard testing panel for medical cotton-linen includes Staphylococcus aureus (ATCC 6538) as the Gram-positive representative. This is the classic hospital-acquired infection pathogen, responsible for wound infections and surgical site complications. We also test against Klebsiella pneumoniae (ATCC 4352) as the Gram-negative representative. Gram-negative bacteria have a more complex double-membrane cell wall that is more resistant to many anti-bacterials. A finish that kills Staph easily can fail miserably against Klebsiella. For fungal control, we test against Candida albicans (ATCC 10231), a yeast that causes opportunistic infections in immunocompromised patients. Our standard finish achieves >3.0 log reduction against all three organisms. For specialized wound-care applications, we have also tested against the antibiotic-resistant strains MRSA (Methicillin-resistant Staphylococcus aureus) and VRE (Vancomycin-resistant Enterococcus), with results above 3.0 log reduction. This broader pathogen panel gives our hospital partners the confidence that our fabric is part of their infection control strategy, not just a passive textile. The rationale behind selecting specific indicator organisms for textile anti-microbial testing is a specialized topic within medical microbiology, and the educational resources available through the Society for Healthcare Epidemiology of America website provide excellent context for understanding why testing against Klebsiella and MRSA is clinically relevant.
What Regulatory Certifications Support Our Medical Cotton Linen Claims?
A test report from our own lab is not a certification. A certificate from an independent, ISO 17025 accredited third-party laboratory is. In the medical textiles world, you cannot self-declare compliance. The hospital's procurement department will demand documentation that proves your anti-bacterial claims have been independently verified, your chemical safety has been toxicologically assessed, and your manufacturing facility operates under a recognized quality management system. If you can't produce this paperwork within 24 hours of a request, your fabric doesn't make the approved vendor list. I learned this the hard way in 2018 when a UK NHS supplier asked for our medical device dossier, and I didn't have it ready. We lost the contract. Since that day, I've maintained a complete, current, and externally audited regulatory documentation package for our medical fabric range. Here's what's in it, and why each certificate matters.

Why is OEKO-TEX Standard 100 Class I essential for patient-contact cotton linen?
OEKO-TEX Standard 100 is a chemical safety certification. It tests the finished fabric for a comprehensive list of harmful substances, including heavy metals, formaldehyde, phthalates, pesticides, and chlorinated phenols. The test criteria are based on the intended use of the textile. Class I is the strictest category, intended for textile items for babies and toddlers under three years old. For medical patient-contact fabrics, Class I is the de facto requirement because the skin of immobile or immunocompromised patients can be as sensitive as a baby's.
Our anti-bacterial medical cotton-linen holds OEKO-TEX Standard 100 Class I certification. This means the silver-ion and QAC finish has been tested and cleared for direct, prolonged skin contact. The certification also verifies that the finish does not leach harmful levels of any regulated substance. I've seen medical fabrics that pass the bacterial kill test but fail the chemical safety test because the anti-bacterial agent is cytotoxic to human skin cells. A high log reduction against bacteria means nothing if the fabric gives the patient contact dermatitis. OEKO-TEX certification closes that safety loop. For brands, having this certificate means their own finished product can carry the OEKO-TEX label, which is a powerful consumer trust signal in the European and North American healthcare markets. The OEKO-TEX Standard 100 certification page on the official OEKO-TEX website provides the complete list of regulated substances and the testing criteria, which I encourage every medical brand buyer to familiarize themselves with before evaluating any fabric supplier.
Does our medical cotton-linen comply with EU Medical Device Regulation (MDR) 2017/745 for Class I devices?
The EU MDR 2017/745, fully in effect since May 2021, reclassified many textile-based medical products. A reusable surgical gown, a patient positioning drape, or a wound-care wrap made from our fabric may fall under Class I medical device classification. As the fabric manufacturer, we are not the legal device manufacturer—the brand that cuts and sews the garment is. But the garment brand relies on us, the material supplier, to provide the biocompatibility data, the anti-microbial efficacy data, and the material traceability that their technical file requires.
Our medical cotton-linen is produced under a quality management system aligned with ISO 13485, the standard for medical device manufacturing. We maintain full batch traceability from yarn lot to finished fabric roll. We provide a material compliance statement that includes the results of cytotoxicity testing (ISO 10993-5), skin irritation testing (ISO 10993-10), and sensitization testing (ISO 10993-10) conducted by an independent GLP-certified laboratory. These are the exact data points a medical device manufacturer needs to include in their MDR technical documentation. When a Dutch medical apparel brand asked us for MDR support documentation in March 2026, we sent them a 120-page dossier within 48 hours. They told me no other fabric supplier they had approached could provide even half of that documentation. That comprehensive regulatory readiness is not an accident. It's an investment I made because I want our fabric to be the path-of-least-resistance choice for medical brands navigating the EU regulatory environment. The full scope of MDR requirements for textile-based medical devices is complex, and the European Commission's official Medical Device Regulation guidance documents are the definitive source that we align our documentation package with.
Conclusion
Anti-bacterial finishing on medical cotton-linen is not a coating you spray on as an afterthought. It's a chemically engineered, independently tested, and regulatorily documented system that we've built into the fiber structure itself. I've shown you the dual-action chemistry today: the fast-kill QACs that rupture bacterial membranes on contact, and the sustained-release silver ions that keep killing through 50 laundry cycles and 20 autoclave sterilizations at 134°C. I explained why our silane-based carrier matrix doesn't hydrolyze under steam like the cheap acrylic binders that most mills use, and why our fabric retains 88% of its tensile strength after two dozen autoclave cycles when ordinary medical linens are falling apart.
I walked you through the ISO 20743 and AATCC 100 testing protocols, and why we test against Staphylococcus, Klebsiella, and Candida—not just one easy-to-kill bacterium. I showed you the regulatory scaffolding that supports every claim we make: OEKO-TEX Class I certification for direct patient skin contact, ISO 10993 biocompatibility data for cytotoxicity and skin irritation, and a quality management system aligned with ISO 13485 so our brand partners can compile their MDR technical files without fighting their own supply chain for data. The German scrub brand that switched to us after their previous finish failed at 30 washes now has a fabric that still kills 99.9% of bacteria after 50. The Dutch medical apparel company that needed MDR documentation got a 120-page dossier in 48 hours.
Medical fabric is a promise. The promise is that this textile, when it touches a patient's skin in a vulnerable moment, will not become a vector for infection. That promise is too serious to be left to a spray-on silver rinse and a vague marketing claim. We back it with chemistry, with testing, and with paperwork.
If you're developing a medical apparel or healthcare textile product that needs a validated anti-bacterial cotton-linen fabric with full regulatory support, reach out to our Business Director Elaine at elaine@fumaoclothing.com. She can send you a sample yardage with the current ISO 20743 test report and OEKO-TEX certificate. She can schedule a video review of our dedicated medical finishing line and our batch traceability system. Or she can connect you with our regulatory affairs consultant to discuss the MDR documentation package for your specific Class I device application. Let's make a fabric that helps hospitals heal, not hurt.